Introduction
Rotator cuff tears or ruptures are among the most common musculoskeletal injuries, with a prevalence of 20% in the general population(1). Larger lesions are associated to poorer functional outcomes and greater postoperative structural failure rates(2,3). Of all rotator cuff ruptures, approximately 20% are massive ruptures(2) that pose a challenge due to their high re-rupture rate of between 18-94%, and their potential irreparability(4).
But what is massive rotator cuff rupture, and what are the criteria for considering it to be irreparable? The truth is that both terms have evolved over time, and although they are intimately related, they are not synonymous. While most irreparable ruptures are massive, some are not. In contrast, many massive ruptures are reparable despite the fact that the term "massive" has connotations of repair difficulty(5).
Many factors need to be taken into account for both the diagnosis and treatment of irreparable massive rupture (IMR) of the rotator cuff, such as the size of rupture, its retraction, the affected tendons and the exploratory findings in relation to them, the degree of adipose or fatty infiltration, the presence or not of degenerative joint findings, the age of the patient, and the physical demands.
The present study offers a review of the concept of IMR of the rotator cuff, with special attention to those lesions that affect the posterosuperior (supraspinatus-infraspinatus) cuff, their classification, and the typical physical exploratory findings.
Definition and diagnostic tests
Massive ruptures
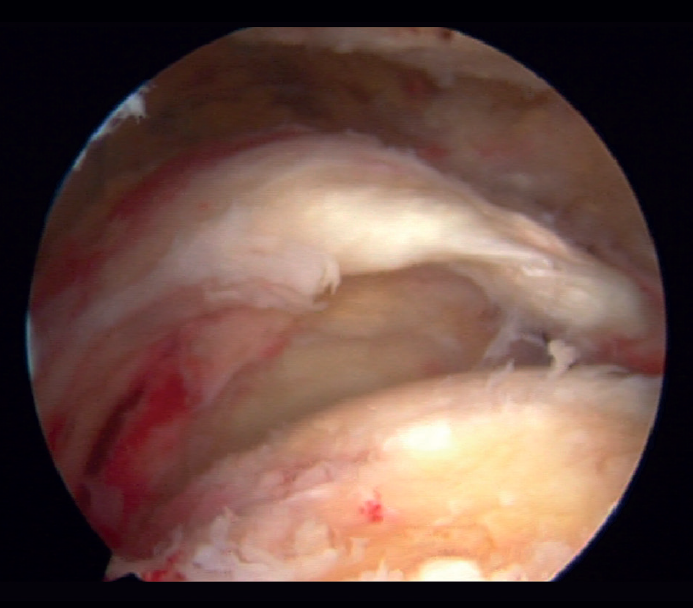
Different definitions of massive rupture of the rotator cuff (MRRC) have been proposed over time. Cofield defined them as lesions measuring 5 cm or more in diameter(6), while according to Gerber et al.(7) they involve the complete deinsertion of two or more tendons, exposing the tuberosities - a circumstance easily identifiable during surgery (Figure 1). On the other hand, Davidson and Burkhart(8) defined such lesions as retracted ruptures measuring at least 2 cm in length in the sagittal plane and with a width of 2 cm in the coronal plane - being identifiable preoperatively by means of magnetic resonance imaging (MRI). However, these definitions may result in bias due to differences in size between patients or the position of the arm at the time of measurement, and they moreover fail to distinguish between different patterns of rupture and do not predict function of the injured shoulder. Accordingly, Ladërmann et al.(9) considered that in addition to the number of damaged tendons, at least one of the two must be retracted more medial to the humeral head - this corresponding to supraspinatus grade 3 retraction in the coronal plane according to the classification of Patte(10), which adds more objective three-dimensional value to the measurement (Figure 2). Lastly, Schumaier et al., involving a group of experts, recently published a consensus document defining massive ruptures as those that are retracted to the margin of the glenoid cavity in the coronal or axial plane and/or present exposure of two-thirds of the greater tuberosity footprint in the sagittal plane(11).
Once MRRC has been identified, it can be subclassified according to the classification of Collin et al.(12), which divides the rotator cuff into 5 components: inferior subscapularis, superior subscapularis, supraspinatus, infraspinatus and teres minor, ordered from anterior to posterior. In relation to these components, rotator cuff ruptures are classified into 5 types:
- Type A: injuries of the supraspinatus and superior subscapularis.
- Type B: injuries of the supraspinatus and entire subscapularis.
- Type C: injuries of the supraspinatus, superior subscapularis and infraspinatus.
- Type D: injuries of the supraspinatus and infraspinatus.
- Type E: injuries of the supraspinatus.
This classification, which is a novelty due to its anatomical division into 5 parts, not only classifies massive ruptures in relation to the damaged parts but also in relation to shoulder function - specifically active elevation, which is a concept we will examine in the section on exploration.

Irreparable ruptures
The concept of MRRC irreparability remains controversial, and given the important technological advances in relation to implants, suture resistance, interval slide techniques(13) and techniques for fixation and load distribution in repair(14,15), the term "irreparable" is still evolving. In addition, the possibility of correct repair does not necessarily imply correct healing or functional improvement of the shoulder. Hence, the making of decisions in relation to MRRC is extremely arduous and complex, and requires many factors to be taken into account - making it difficult to predict the reparability of rupture.
The most determining prognostic factor in the therapeutic algorithm is the degree of fatty infiltration of the muscle bellies as postulated by Goutallier et al.(16). This classification assesses the degree of fatty infiltration from a computed axial tomography (CAT) axial scan of the shoulder. Grade 0 corresponds to the absence of fatty infiltration. Grade 1 is characterized by small adipose inclusions. Grade 2 still presents more muscle than adipose tissue, while in Grade 3 both components are present in equal proportions (50%). Lastly, Grade 4 is characterized by the presence of more fat than muscle. Grades 3 and 4 show the poorest prognosis, though the repair of MRRC with grade 2 and 3 fatty infiltration and a supraspinatus tendon length of less than 15 mm exhibit a failure rate of up to 92%. However, if the length of remaining tendon is over 15 mm, the failure rate drops to 33%. In this respect, Meyer et al.(17) concluded that the combination of the classification of Goutallier with the size of the tendon stump appears to be a powerful predictor of MRRC reparability.
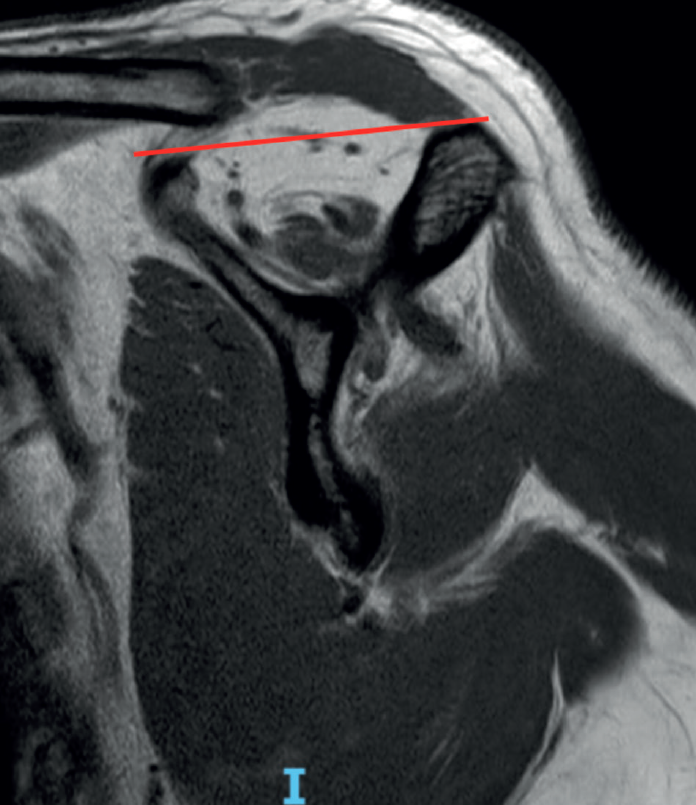
The fish backbone sign(18), in which the muscle belly presents a veined or streaky pattern reminiscent of a fish backbone, is another indicator of fatty infiltration of the muscle belly in the axial axis of the CAT scan, and is equivalent to Goutallier grade 3. The classification of Goutallier has been validated in MRI, and measurement is made in the sagittal section where the scapular spine comes into contact with the body of the scapula, producing a "Y" shaped image(19). Another predictor of irreparability and also an indicator of advanced fatty infiltration is the tangent sign of Zanetti et al.(20). According to the authors, advanced fatty infiltration is present when on tracing a line from the upper margin of the coracoid process to the upper margin of the scapular spine in the same sagittal section of an MRI scan in which a "Y" image is obtained, there is no cut in the muscle volume of the supraspinatus (Figure 3). When measuring in the sagittal view of an MRI scan, we must take into account that a healthy muscle presenting some retraction may simulate greater than real fatty infiltration, and conversely, the muscle may seem normal postoperatively, suggesting that the fatty infiltration has reverted, when in fact it is only healthy but retracted muscle. Fatty infiltration is irreversible and progressive, and although minor improvements have been observed after the repair of these tendons(21), the results are generally poorer than in situations of low grades of adipose atrophy, especially of the infraspinatus(22). Thus, one of the aims of early repair (within 2.5 years from symptoms onset) of rotator cuff injuries is to prevent the condition from progressing to higher grades of adipose atrophy associated with irreversible loss of function and the concept to irreparability(23).
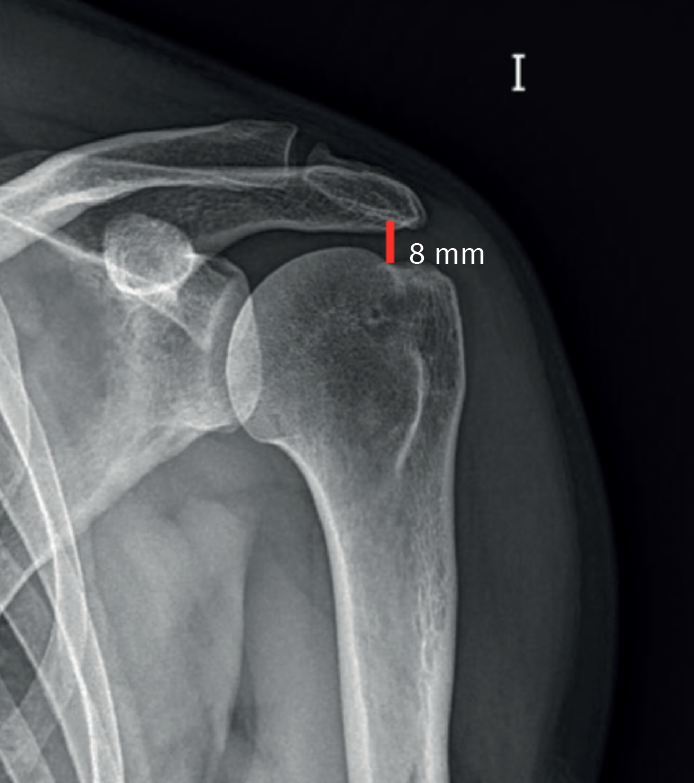
Another indicator of irreparability is the acromiohumeral distance (AHD). This is measured according to the classification proposed by Hamada et al. in 1990(24) (and modified in 2011)(25) for MRRC based on an anteroposterior plain radiograph of the shoulder, comprising 5 grades: in grade 1, AHD measures 6 mm or more (Figure 4); in grade 2 it narrows and measures 5 mm or less; in grade 3 acetabularization of the acromion is observed secondary to ascent of the humeral head; grade 4 is subdivided into grade 4A with narrowing of the glenohumeral joint space without acetabularization of the acromion and grade 4B with acetabularization; and lastly grade 5 consists of humeral head collapse. An AHD of less than 6 mm is considered to be an independent predictor or irreparability. Thus, those cases of MRRC corresponding to Hamada grade 2 or higher are considered to be irreparable.
The mediolateral magnitude of the rupture has also been postulated as an independent irreparability factor. Thus, ruptures with a mediolateral size of 47.4 mm were considered to be irreparable in a sample of 758 patients subjected to multivariate logistic regression analysis(26). In this same study, those lesions jointly affecting the supraspinatus, infraspinatus and subscapularis were also regarded as irreparable.
The degree of tendon retraction is not an irreparability indicator in itself. In this sense, it is important to take into account that L-shape or inverted L-shape ruptures may present a greater than real mediolateral size in some coronal MRI sections, simulating retraction grade 3 of the Patte classification, when in fact their true size is smaller and they may be reducible and reparable(27) - as can also occur with large retracted ruptures produced in the context of acute trauma(28).
Chronic pseudo-paralysis (with no recent acute event) is also an independent indicator of irreparability(26), with the pseudo-paralytic shoulder being understood as a shoulder with an elevation in active flexion < 90°, with complete passive joint balance, no neurological involvement and not caused by pain but characterized by genuine functional involvement (Figure 5)(12). The pseudo-paralytic shoulder is one of the possible manifestations of MRRC and will be addressed in the section on physical examination.

The age of the patient, physical activity, the time from onset of the lesion and concomitant conditions such as diabetes or smoking, are secondary factors which along with those described above must be taken into account in the decision making algorithm(5).
Physical examination and classification
Clinically, patients with MRRC may be asymptomatic(5). This is because the torque between the non-injured rotator cuff, the deltoid muscle and the rest of the periscapular muscles is balanced. In other words, despite the damage, the rotator cuff is able to exert compression force between the humeral head and the glenoid cavity, thus generating a stable fulcrum on which the deltoid muscle and the periscapular muscles are able to displace the humeral head with respect to the glenoid cavity(9).
This is possible thanks to the rotator cable, which is a thickening of the cuff acting as protection of the critical zone of this front to traction. It has been compared with a suspension bridge that distributes the forces among the supporting pillars and which, in the case of the rotator cuff, would be its anterior and posterior insertion(29). The more anterior insertion of the rotator cable divides around the bicipital groove, and its posterior pillar comprises the 50% lower portion of the insertion of the infraspinatus, which would explain why patients with ruptures of the rotator cuff between these pillars are able to maintain good active joint balance (30) and why even partial repairs of the rotator cuff achieve good functional outcomes(31).
When patients with MRRC present symptoms, they often experience typically nocturnal pain and pain with activities requiring them to raise the arm above head level, though the severity of pain is not related to lesion grade(32). The functional deficits that we can identify at physical examination are correlated to the location of the lesion. Consequently, those patients with complete subscapularis injuries will produce positive belly-press(33) and lift off(34) tests and a positive lift off lag sign(35). Supraspinatus insufficiency, present in all massive ruptures according to Collin et al.(12), is normally associated to positive Jobe(36) and drop arm(37) maneuvers, with a decrease in external rotation strength with the elbow in approximation(9). Damage to the posterosuperior cuff is usually associated with a positive external rotation lag sign, which has high sensitivity and specificity(38). The horn blower sign, which implies that the patient cannot maintain external rotation with the shoulder in 90° abduction, offers high sensitivity and specificity in diagnosing posterosuperior cuff lesions that affect the tendon of the teres minor muscle(39).
Asymptomatic patients in the context of MRRC, apart from all the already mentioned tests, and due to involvement of the rotator cable, with the consequent impossibility of compensating torque, may present a pseudo-paralytic shoulder which - as already described - is characterized by elevation in active flexion of < 90º in the absence of neurological damage and stiffness. If doubts arise during exploration as to whether the functional limitation is caused by pain, we can resort to a subacromial anesthetic test as a diagnostic strategy, where a genuine pseudo-paralytic shoulder would continue to present an elevation defect(40). It must be commented that the term pseudo-paralysis has still not been fully defined, for although the most widely accepted definition is that already mentioned above, some authors limit the term to shoulders with completely abolished active elevation, while others consider an elevation of less than 45º, always in the context of chronicity(41). In contrast, thanks to the study published by Collin et al.(12), we do know that the rupture patterns most associated with pseudo-paralysis are B (involvement of the supraspinatus + complete subscapularis with 80% pseudo-paralysis), C (superior subscapularis + supraspinatus + infraspinatus with 45% pseudo-paralysis) and E (supraspinatus + infraspinatus + teres minor with 30% pseudo-paralysis).
In 2018, Boileau et al.(42) established a classification of shoulders with MRRC according to their functional imbalance:
- Group I or PLEA (painful loss of elevation [active]): loss of active elevation due to pain. This is not a pseudo-paralytic shoulder, because the pain subsides with a subacromial anesthetic test, and muscle balance is preserved.
- Group II or ILEA (isolated loss of elevation [active]): pseudo-paralytic shoulder with loss of elevation due to imbalanced torque.
- Group III or ILER (isolated loss of external rotation): this is not pseudo-paralysis as such, since there is only loss of external rotation due to horizontal alteration of muscle balance.
- Group IV or CLEER (combined loss of active elevation and external rotation): pseudo-paralytic shoulder with deficit of both active elevation and external rotation. It is divided into two types:
- CLEER 1: deficit of both movements, fundamentally deficit of active elevation, with some preservation of external rotation.
- CLEER 2: abolished active elevation and external rotation.
In this classification, the authors assigned a treatment option of choice to each group; this will not be addressed here, however, as it falls outside the scope of this monographic article.
Another term, CLEIR, introduced by Kany et al.(43), involves the presence of a pseudo-paralytic shoulder with combined active elevation and external rotation deficit and Goutallier grade III atrophy.
Conclusions
Although the terms massive rupture and irreparable rupture are sometimes used indistinctly, they are not synonymous, and their definition has evolved over time. The most widely accepted definition refers to massive ruptures as those that are retracted to the margin of the glenoid cavity in the coronal or axial plane and/or present exposure of two-thirds of the greater tuberosity footprint in the sagittal plane. The most determining factor defining irreparability is the degree of fatty infiltration of the muscle belly according to the classification of Goutallier, with grades 3 and 4 presenting the poorest prognosis. Other factors that must be taken into account in defining rupture irreparability are an acromiohumeral distance < 6 mm, mediolateral rupture size 47.4 mm, Patte retraction grade 3, combined involvement of the supraspinatus, infraspinatus and subscapularis, and pseudo-paralytic shoulder in the absence of an acute event.
Patients with irreparable massive cuff rupture may remain asymptomatic provided the shoulder presents a balanced torque. If symptoms are present, the functional deficits are related to the damaged tendon structures. One possible manifestation is pseudo-paralytic shoulder, which is most often seen in Collin type B, C and E ruptures. Lastly, cases of irreparable massive rotator cuff rupture are classified into 5 groups according to the deficit involved: PLEA, ILEA, ILER, CLEER and CLEIR.




