Introduction
Rotator cuff disease is a frequent clinical problem, with a high incidence of degenerative cuff ruptures in people aged 50 years or older(1). Despite the high prevalence of rotator cuff ruptures, controversy persists regarding the optimum treatment for such injuries(2). Surgery for posterosuperior rotator cuff rupture is an option of choice. However, depending on the characteristics of the rupture, the problem may be regarded as irreparable, or we may face repair failure. In this respect, the reported failure rate ranges from 17-69% of all operated cuffs(3). In either situation, a non-surgical approach to posterosuperior rotator cuff rupture remains the initial recommendation in patients of this kind. In addition, many patients with irreparable posterosuperior rotator cuff ruptures present comorbidities, and in such cases surgery may be contraindicated or not recommended. For this reason, rehabilitation might be the only management option available in these cases.
There is agreement that most patients with irreparable rotator cuff ruptures should first receive non-surgical treatment based on pain control (addressed in another chapter of this monograph), muscle strengthening, and kinematic, scapular and stability re-education(4).
This treatment objective is addressed by rehabilitation and physical therapy, the main elements of which are physiotherapy and electrophysical therapies. Physiotherapy seeks to improve the range of motion, strength and stability of the shoulder, while electrophysical therapies focus on managing pain and inflammation.
Such conservative management with rehabilitation and physical therapy affords variable success rates, depending on the characteristics of the patients and the characteristics of the affected tendons, as well as on the already established dysfunctions such as ascent of the head of the humerus or scapular dyskinesia(5).
The present study describes the current concepts in rehabilitation and physical therapy, the different characteristics of the available rehabilitation protocols, and the clinical results obtained in patients with irreparable rotator cuff ruptures.
Anatomy and biomechanics of the shoulder with irreparable rotator cuff injury
Torque is a moment of force generated by two equal, non-collinear, parallel but opposite forces. In other words, rotation around a joint axis is accompanied by obligatory rotation over another joint axis, and these movements are coupled together. The muscles of the scapular girdle interact to generate specific torques that maintain collinear instantaneous centers of rotation between the humeral head and the glenoid fossa(6). Inman et al. noted that during raising of the arm, the deltoid muscle and the rotator cuff tend to act synchronically as a torque mechanism to allow balanced movement through the glenohumeral joint(7).
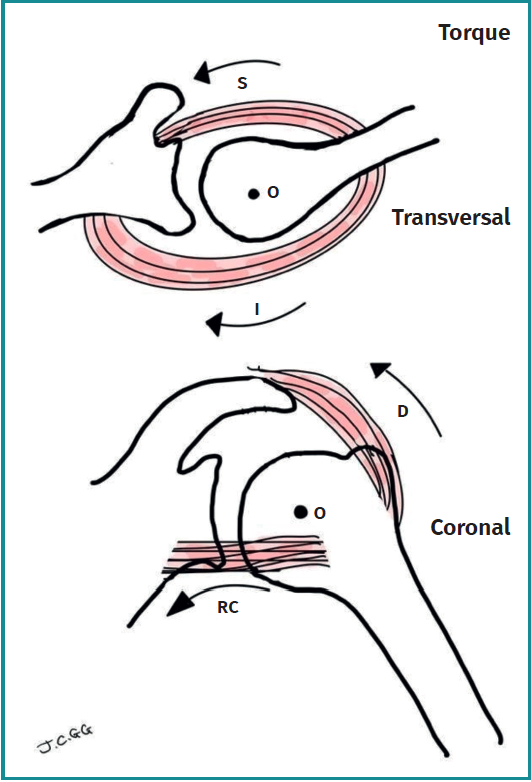
The origin of the deltoid muscle is located above and external to the glenohumeral joint, with its distal insertion in the humeral diaphysis. As a result, the total forces produced at the start of abduction and at the initial 45º of elevation are mainly vertical, generating a significant ascending shear effect. The force patterns of the rotator cuff muscles contrast with those of the deltoid muscle. The supraspinatus, by originating horizontally, mainly generates compression force in the joint. This force helps to center the humeral head in the glenoid cavity during elevation or raising of the arm, and counters the superiorly guided force of the deltoid muscle. Even more relevantly, the force resulting from the subscapularis, the infraspinatus and the teres minor is mainly directed downwards (i.e., exerting depression upon the humeral head), and opposes the upward force of the deltoid muscle(6)(Figure 1).
As described by Inman et al., the torque in the coronal plane involves deltoid muscle opposition against the most posteroinferior portion of the rotator cuff (i.e., infraspinatus and teres minor). The torque in the transverse plane involves the anterior or subscapular cuff, balanced against the posterior rotator cuff, i.e., the infraspinatus and teres minor(7).

In order to ensure adequate shoulder function, collaboration is needed between the acromioclavicular, glenohumeral and scapulothoracic joints, together with synchronization of the muscles involved. Elevation and protraction of the scapula is an important element in elevation of the arm and functions so that the acromion leaves space for the humeral head. This scapulothoracic force pattern is conformed by the elevator of the scapula and the anterior serratus muscle, balanced against the upper and lower trapezius. Weakness of any of these muscles can alter the normal scapular dynamics and balance, and lead to abnormal movement.

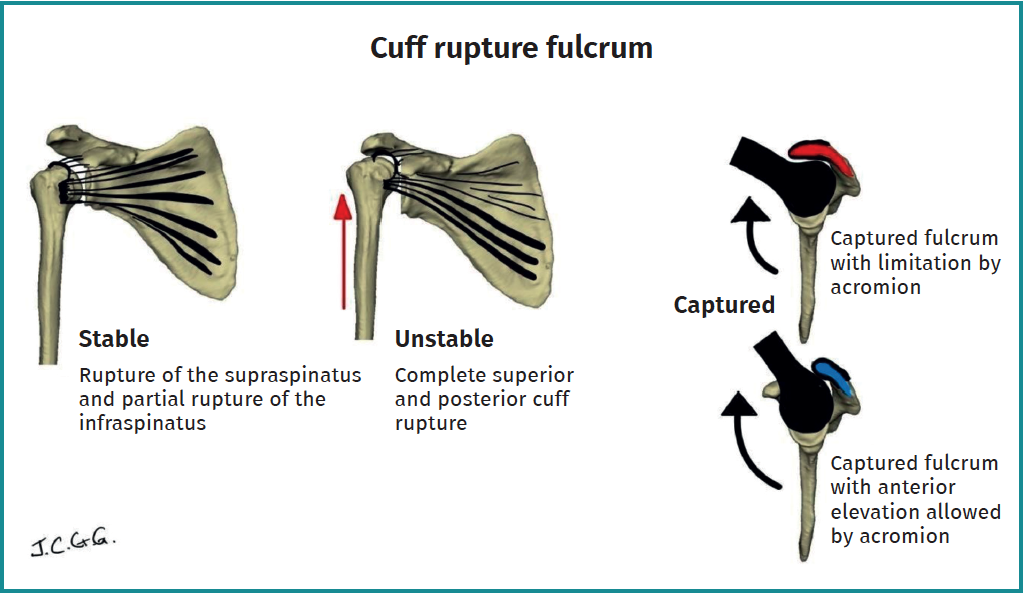
Burkhart identified three different motion patterns in irreparable rotator cuff ruptures, based on a fluoroscopic study. Firstly, he identified a "stable" pattern in patients with a normal range of motion of the shoulder. In this case the rotator cuff is able to keep the humeral head adequately centered in the glenoid cavity. Secondly, he identified an "unstable" pattern characterized by anterior and superior translation of the humeral head, without active shoulder elevation. Thirdly, he described a "captured" pattern. In this situation, where the rotator cuff is unable to keep the humeral head centered in the glenoid cavity, the deltoid muscle is strong enough to allow active elevation of the shoulder, displacing the center of rotation of the humeral head towards the lower surface of the acromion(8)(Figure 2).

Scapular dyskinesia is often seen in irreparable ruptures. Scapular dyskinesia is characterized by alteration of the normal muscle activation patterns of the periscapular musculature, and is associated with the inhibitory effect of pain caused by irreparable rotator cuff rupture. Such pain limits individual muscle activation capacity(9). Scapular dyskinesia manifests as an adaptive and compensating mechanism to allow mobility of the affected arm, despite limited or absent activation of the rotator cuff(8). This is achieved through early activation of the periscapular muscles, seeking to stabilize the scapula and afford a stable base for the glenohumeral movements during elevation of the arm(10).

The biomechanical basis for conservative management is to restore as far as possible the normal muscle balance around the shoulder, with specific attention to improving the efficiency of the depressors of the humeral head, without activating the deltoid muscle. This muscle balance is achieved by strengthening the significant depressors of the humeral head and strengthening the scapular elevators. It must be noted that before strengthening the shoulder muscles, the shoulder must have a full range of motion(5).
Functional outcomes of physiotherapy in irreparable ruptures
Few studies have investigated the efficacy of rehabilitation treatment specifically in the subgroup of patients with irreparable posterosuperior rotator cuff rupture. Of the articles that have evaluated the global outcome of rehabilitation therapy in cuff disease, mention must be made of the study conducted by a group of shoulder surgeons (MOON Shoulder Group)(11) in 422 patients, with the inclusion of all types of atraumatic ruptures of the posterosuperior cuff, subjected to physiotherapy (home exercises assisted by a therapist as required), and with a minimum follow-up of 12 months. In this series, conservative management allowed 75% of the patients to not need surgery.
Collin et al.(12) carried out a prospective study including 45 patients with irreparable massive rotator cuff injuries and with pseudo-paralysis. They classified the patients according to the anatomical location of the rupture, and grouped them according to the tendon or tendons affected. Following the classification, a protocol was applied, focused on the alleviation of pain, strengthening of the stabilizers of the scapula, and the recovery of proprioception, with a minimum follow-up of two years. The aim of this study was to establish a specific physiotherapy protocol comprising 5 sessions for these patients, with special emphasis on strengthening the muscles in charge of stabilizing the scapula. They found that those patients with massive ruptures involving the tendons of the subscapularis and supraspinatus (anterosuperior cuff) presented poorer outcomes than those with massive ruptures of the supraspinatus and infraspinatus (posterosuperior cuff). No patient with massive rupture of the anterior cuff was able to achieve flexion of more than 60º, in contrast to those with massive rupture of the posterosuperior cuff. The authors concluded that anterior cuff injury is a prognostic factor for the development of pseudo-paralysis and a poor clinical course with rehabilitation therapy. Among the patients with massive posterior rupture, 24 did achieve flexion of over 160º and improved scores on the Constant functional scale, and were thus more amenable to rehabilitation therapy. They also concluded that patients with the involvement of three or more tendons had poor outcomes in comparison with individuals presenting fewer than three affected tendons. These observations suggest that the anatomical location of massive ruptures of the rotator cuff may influence the outcomes of rehabilitation. Furthermore, emphasis was placed on the importance of focusing rehabilitation efforts on strengthening the muscles in charge of stabilizing the scapula, in order to improve shoulder function in these patients.

Another study by Vad et al.(13) investigated the prognostic factors in massive / irreparable rotator cuff injuries and their relation to the outcomes of different types of treatment. A total of 108 patients were included, of which 40 received conservative treatment. The study identified a number of factors indicative of a poor prognosis in irreparable lesions. These factors included the presence of glenohumeral osteoarthrosis, reduction of passive range of motion, superior displacement of the humeral head, the presence of muscle atrophy and loss of strength in rotation / abduction (< 3 on the Daniels scale). The results of the study showed that those patients with three or more of these factors indicative of a poor prognosis had poorer outcomes with any type of treatment, including conservative management. This suggests that the presence of multiple indicators of a poor prognosis can negatively influence the response to treatment, independently of the therapeutic approach adopted.

Yian et al.(14) carried out a study involving 30 patients with irreparable rotator cuff ruptures, applying a physiotherapy program based on non-supervised re-education of the anterior deltoid muscle during a period of three months, and with a follow-up period of two years. The results were disappointing, with a success rate of 40%. The mentioned study also analyzed different factors that could influence the results of the deltoid muscle re-education program, such as patient age, gender, pain, range of motion, pseudo-paralysis, the number of affected rotator cuff tendons, the presence of associated rupture of the subscapularis or teres minor, and the presence of glenohumeral osteoarthritis. However, no statistically significant association was observed between any of the factors, with the exception of active range of motion. The authors concluded that those patients with flexion of less than 50º before the start of the anterior deltoid muscle re-education program had a poor prognosis with rehabilitation treatment. Those individuals with limited flexion could be less likely to achieve good outcomes with rehabilitation therapy. However, it is important to taken into account that this study involved a limited number of patients, and further research in needed to confirm these findings and to better understand the factors that influence the results obtained with rehabilitation therapy in such lesions.
Yoon et al.(15) conducted a 5-year study of 110 patients with irreparable massive ruptures affecting at least two tendons (supraspinatus and infraspinatus), fatty infiltration (Goutallier stage III or IV), and hypotrophy evidenced by magnetic resonance imaging. The patients were divided into 2 groups. Group A presented an intact tendon of the subscapularis and a hypertrophic teres minor, while group B presented injuries of the subscapularis and/or teres minor. Rehabilitation therapy consisted of passive mobilization to maintain glenohumeral mobility, along with strengthening of the deltoid muscle. The conservative management failure rate in group A was 43%, versus 68% in group B. Furthermore, percentage conversion to surgery was 39% in group A and 66% in group B. These findings suggest that patients with an intact tendon of the subscapularis muscle and a hypertrophic teres minor have lower failure rates with conservative treatment and lower rates of conversion to surgery compared with those presenting injuries of the subscapularis and/or teres minor. However, it is important to taken into account that this study was based on a specific classification of rotator cuff lesions, and that the results may vary depending on other individual patient factors.
Characteristics of the rehabilitation protocols
There are no universally standardized protocols. Globally, the protocols include changes in lifestyle, manual manipulation, physiotherapy, electrotherapy and coadjuvant treatment with antiinflammatory drugs and the infiltration of corticosteroids in the subacromial space(14,16,17). Different models are accepted, including both supervised and non-supervised physiotherapy. Both options have been shown to improve the functional scores, though they have not been directly compared with each other(5).

Many of the published protocols(17,18,19,20) suggest that the rehabilitation program should include supervised therapy and an exercises program to be applied at home. Therapy should be supervised by a physiotherapist to ensure that the exercises are correctly carried out, following the frequency and duration prescribed by the rehabilitating physician. It is advisable to carry out the physiotherapy program at least 2-3 times a week and for a minimum of 12 weeks.
Some rehabilitation programs focus on strengthening the deltoid muscle to compensate the loss of function of the rotator cuff and allow active abduction of the shoulder. Levy et al.(17) showed that a program involving exercises to strengthen the deltoid muscle suffices to reduce pain, improve function and increase the range of motion in 90% of the patients with irreparable rotator cuff rupture.
Our proposed physiotherapy protocol, based on the different published protocols(17,18,19,20) for treating irreparable rotator cuff ruptures, can be structured into three phases, as detailed below.
Phase 1: improvement of passive range of motion and reduction of pain (2-4 weeks)
This phase begins with flexion and passive external rotation exercises of the shoulder. The pain produced by the physiotherapy program after each session should be mild to moderate, with a maximum duration of pain of 12 hours(19).
In this phase we can add manipulation techniques such as posterior glenohumeral mobilization (Figure 3) or scapular mobilization (Figure 4), which reduce stiffness and afford an analgesic effect. These techniques each require 8-10 repetitions, with a 30-second rest between them, and it must be taken into account that no type of manipulation offers evidence of being superior to the rest.
Phase 2: progressive strengthening (4-8 weeks)
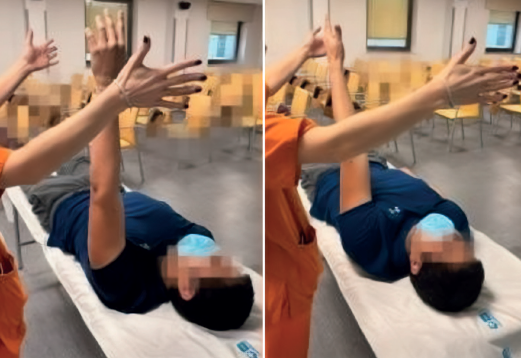
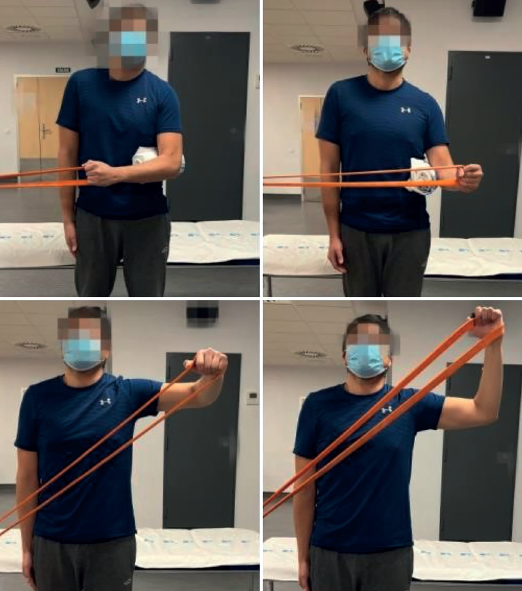
After achieving a greater passive range of motion, the patient enters the assisted active exercises rehabilitation program (Figures 5 and 6) on a gradual basis, followed by active exercises (Figure 7). Once the patient achieves a complete active range of motion, we introduce resistance exercises with small weights (< 1 kg) (Figure 8); there are specific resistance exercises for the deltoid muscle (Figure 9) and for the teres minor (Figure 10). The patients are instructed to perform the movements in a controlled manner for 5 minutes or until muscle fatigue appears. It is advisable to perform the strengthening exercises 3-5 times a day. If the patient is unable to comfortably perform the active exercises in the standing position, they can be carried out in supine or lateral decubitus (Figure 11) using light weights.
Phase 3: proprioception and scapular stabilization (8-12 weeks)
Patients with rotator cuff rupture present increased superior scapular rotation; for this reason proprioception and scapular stabilization exercises are needed to improve control and coordination of the muscles around the scapula. These exercises usually involve retraction, protraction, elevation and depression movements of the scapula. It is advisable to perform 10 repetitions of each, three times a day.
It is fundamental to control pain and to adjust the intensity and the duration of the exercises according to the tolerance and response of the individual patient.
Role of electrophysical therapies in the management of irreparable rotator cuff ruptures
Electrophysical therapies are different types of treatment that seek to reduce pain and improve function through an increase in energy (electrical, acoustic, luminous or thermal) in the body. Different modalities are available, such as ultrasound, pulsed electromagnetic fields, extracorporeal shock waves, transcutaneous electrical nerve stimulation (TENS), laser, iontophoresis or phonophoresis(21). They exert their analgesic effect through activation of the A-beta afferent peripheral fibers responsible for blocking pain transmission, in accordance with the gate theory of pain(22,23). However, it has not yet been established which of these therapies is best suited for treating a specific shoulder condition; as a result, their usefulness in application to irreparable rotator cuff ruptures likewise has not been well defined.
A systematic Cochrane review was carried out in 2016 to compile scientific evidence on the use of different electrophysical therapies in disease of the rotator cuff. However, the mentioned review did not specifically address irreparable ruptures and was based on studies with low scientific evidence. It was concluded that no given treatment modality was superior to the rest, or with respect to other treatments such as glucocorticoid infiltration. Mild improvement of the clinical manifestations over the short term can be expected with the use of these therapies, with slightly better performance versus placebo in the case of laser-based therapies, though the available scientific evidence is limited. On the other hand, it should be mentioned that no relevant adverse effects have been reported when using the different electrophysical therapies in the management of shoulder disease(21).
There is uncertainty and a lack of scientific evidence regarding the different treatment modalities based on electrophysical principles, and the isolated use of electrotherapy as sole treatment choice should be avoided. Their use is recommended in combination with other treatments such as surgery, physiotherapy, analgesics and corticosteroid infiltrations(21).
Conclusions
In irreparable rotator cuff ruptures, the physiotherapist may improve the functional scores and quality of life of the patients. In relation to the factors determining the success or failure of physiotherapy, the pattern of rupture appears to exert an influence, in particular the affected tendons that alter the imbalance of the force patterns, as well as the presence of established defects such as ascent of the humeral head or scapular dyskinesia.
Electrophysical therapies in their different modalities act as coadjuvant treatment, and there is no evidence that they are effective when used on an isolated basis.
Attempts have been made to develop a rehabilitation treatment protocol; however, the level of evidence is limited, and the optimum rehabilitation therapy for these patients remains unclear.










