Introduction
Normal shoulder function depends on the combined action of the muscles of the rotator cuff and the deltoid muscle. These muscles act as dynamic stabilizers, centering the humeral head in the course of its movement(1). The forces that intervene in the glenohumeral joint act in pairs and are present in the coronal and the transverse planes(2). The balance in the coronal plane is maintained by means of torque involving the deltoid muscle and the lower cuff, while balance in the transverse plane is maintained by the subscapularis in the lower part and the infraspinatus and teres minor in the posterior part(3,4,5). Any imbalance in torque can alter the normal kinematics of the shoulder and cause loss of function. Tendon transfers were introduced as reconstruction options to restore the anteroposterior balance of torque in the shoulder joint.
Transfer of the latissimus dorsi
Anatomy and biomechanics
The latissimus dorsi is a triangular shaped muscle originating in the posterior portion of the iliac crest, the lumbar fascia, dorsal vertebras T7 to T12, the last four ribs, and in some cases the inferior angle of the scapula. The muscle in turn inserts in the bicipital groove of the humerus. It is innervated by the thoracodorsal nerve (C6-C8), and its function consists of extension, adduction and internal rotation of the arm(6).
Transfer of the tendon of the latissimus dorsi seeks to restore active external rotation of the shoulder in the context of imbalance caused by posterior cuff rupture(7). The first to use this transfer was L'Episcopo in 1936, for treating obstetric brachial paralysis(8). Posteriorly, Gerber used it successfully to treat irreparable massive rotator cuff ruptures(9,10). Transfer of the latissimus dorsi allows us to cover the posterosuperior defect and affords external rotation strength, thereby restoring torque and improving shoulder motion(11). With transfer to the most anterior zone of the greater tuberosity, the function of the latissimus dorsi switches from internal rotation to external rotation. This function is achieved by active muscle contraction but also through a tenodesis effect that exerts passive force to balance the torque. Furthermore, the latissimus dorsi acts as a humeral depressor, opposing its cranial displacement; this allows the deltoid muscle to be more efficient in abduction and anterior flexion of the shoulder(12).
However, despite the functional improvement achieved through transfer of the latissimus dorsi in irreparable posterior ruptures, normal external rotation function of the shoulder is not fully restored. This is mainly because the traction line of transfer of the latissimus dorsi is more vertical than that of the posterior cuff (infraspinatus and teres minor)(7).
Indications and contraindications of transfer of the latissimus dorsi
The success of any surgical technique is largely conditioned by a good indication, though in the specific case of tendon transfer due to irreparable cuff rupture, a good indication is crucial. The outcome can be influenced by many factors. Careful patient selection is therefore required, taking into account the indications and contraindications.
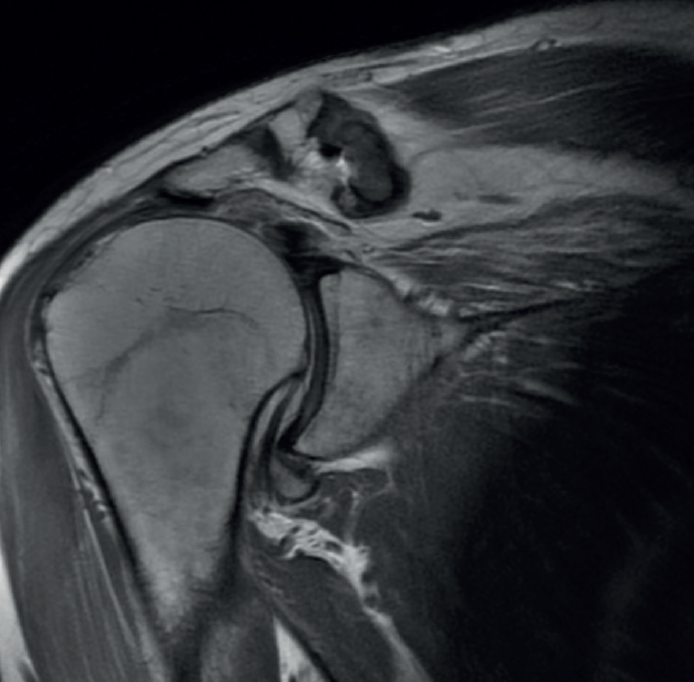
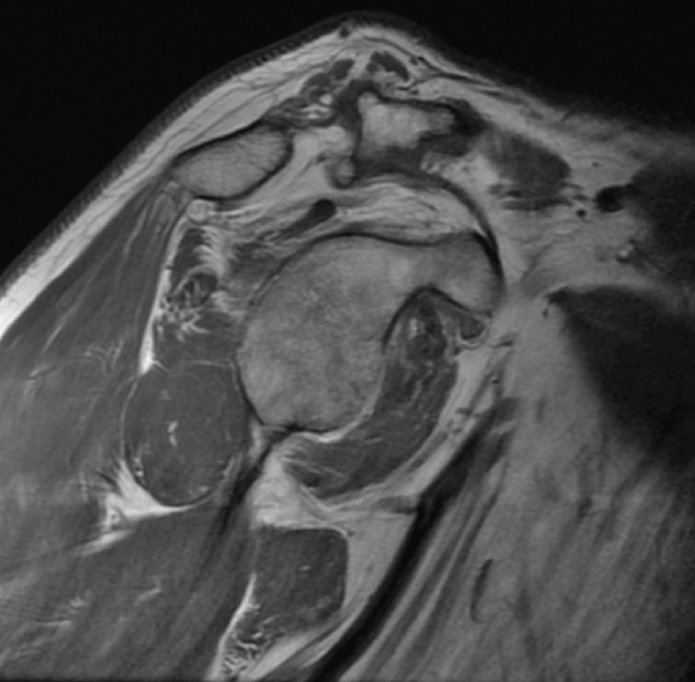
The preoperative evaluation must take a number of aspects into account, including patient age, pain, disability, functional demands and the patient expectations. In this respect, the patient must be duly informed about the expectable functional results. We also must consider other factors that can affect the surgical outcomes, such as patient comorbidities, deltoid muscle and subscapularis function, the integrity of the coracoacromial arch, the presence of arthrotic changes (Figure 1), and the need for the patient to enter prolonged rehabilitation. The main symptoms of massive ruptures of the rotator cuff are typically pain, weakness and loss of mobility(13,14). Irreparable massive ruptures are a common cause of intense pain and often prove extremely disabling for the patient. In general, patients with posterosuperior cuff rupture present reduced flexion-elevation and abduction, and total or partial loss of active external rotation(15,16). A positive external-rotation lag sign and positive hornblower sign are indicative of a deficit of the posterior cuff with the disabling of external rotation, and are associated with irreparable rupture of the teres minor and advanced fatty infiltration(17,18). The appearance of these signs at exploration is associated with poor outcomes of transfer of the latissimus dorsi(13,19). Weakness proves highly variable, and in extreme degrees we observe pseudo-paralysis. Although consensus is lacking, pseudo-paralysis in elevation could be defined as the inability to perform active flexion-elevation of 90º in the absence of nerve damage and with preserved passive mobility. External rotation pseudo-paralysis is defined as the complete loss of active external rotation strength in the presence of unrestricted passive external rotation and the absence of neurological lesions. Some authors consider pseudo-paralysis to be a contraindication to transfer of the latissimus dorsi(20), and is seen to be associated with poor outcomes, since it does not afford the necessary strength to overcome a pseudo-paralytic shoulder and achieve postsurgical elevation(12). Most authors agree that the deltoid muscle must be in good condition in order to perform transfer(21). Irreparable rupture of the subscapularis is an absolute contraindication to this kind of transfer, due to anterior escape of the humeral head when the deltoid muscle contracts in the absence of the subscapularis(9). However, good results can be obtained in partial ruptures of the upper third of the subscapularis that can repaired in the same surgical step(21)(Figures 2 and 3).

The presence of severe osteoarthrosis, above Hamada stage 2(22), or the existence of anterosuperior escape, is considered to be a contraindication to transfer, since both are associated with poor outcomes in transfer of the latissimus dorsi(23,24).
The absolute contraindications are:
- Deltoid muscle paralysis.
- Advanced glenohumeral osteoarthrosis (Hamada 3, 4 or 5).
- Infection.
- Irreparable subscapularis rupture.
- Pseudo-paralysis with elevation < 90º.
- Anterosuperior escape.
The relative contraindications are:
- Elderly patients.
- Fatty infiltration of the teres minor.
- Subscapularis repair under tension.
- Poor bone quality.
- Deficient patient commitment to postoperative rehabilitation.
Surgical technique
Transfer of the latissimus dorsi can be made via an open technique (with double or single incision) or in combination with arthroscopy.
Double incision
The original technique described by Gerber involved a double incision through the axilla for deinsertion of the tendon and superiorly through the deltoid muscle for deinsertion of the latter(9). The operation is carried out with the patient in lateral decubitus. A superior approach is adopted, with a medial incision parallel to the lateral acromion, separating the middle deltoid with a small fragment of the lateral acromion, which allows us to expose and partially repair the rotator cuff, associated to reinsertion of the latissimus dorsi. The axillary approach is performed with the arm in full elevation, through an L-shaped incision at the anterolateral margin of the latissimus dorsi. The latissimus dorsi is located anterior to the teres major, and its tendon is broad and very thin. We dissect the interval between these two muscles and free the insertion in the humerus. Once freed from the humeral insertion, the tendon is reinforced with two high-resistance sutures in Krackow configuration, to prevent possible tearing. Then, the muscle belly is dissected, identifying the neurovascular pedicle to increase mobility. The muscle is transferred through the interval between the deltoid muscle and the infraspinatus and teres minor. The tendon is then fixed in the insertion of the supraspinatus with anchorings, while fixation of the remaining rotator cuff is performed to the medial margin of the tendon. The middle deltoid muscle is repaired in the lateral acromion using transosseous sutures.
Single incision
A less invasive technique is the posterior single incision approach described by Habermeyer(25). The main advantage of this technique is that the deltoid muscle is not deinserted, and the posterior rotator cuff is directly visualized through a V-shaped posterior incision. The main disadvantage is that the anterosuperior rotator cuff cannot be visualized or repaired when necessary. The site of transfer fixation is somewhat more posterior and lateral, in the insertion footprint of the infraspinatus.
Arthroscopy-assisted technique
The technique can be carried out assisted by arthroscopy(26,27) or adopting a fully arthroscopic approach(28), thereby avoiding the damage to the deltoid muscle that may occur during open transfer. With the arthroscope in the posterior portal, we prepare the anterior and lateral portion of the greater tuberosity in the footprint of the supra- and infraspinatus for fixation of the latissimus dorsi. Then, with the arthroscope in the lateral portal, passage between the deltoid muscle and teres minor is established with the synoviotome and vaporizer. We then perform dissection and preparation of the latissimus dorsi through an axillary approach. Next, the tendon is passed between the deltoid muscle (superficial) and the infraspinatus and teres minor (deep), pulling upon the sutures through the anterior portal, and finally fixing the tendon with anchorings.
A mini-open approach was posteriorly introduced for deinsertion of the latissimus dorsi that was used in combination with arthroscopy for transfer and fixation(29). The pedicle of the latissimus dorsi is identified preoperatively by doppler ultrasound, allowing us to perform a minimal axillary incision of about 5 cm with simple dissection, thereby reducing the length of the incision. Tendon fixation is performed via arthroscopy.
Postoperative phase
Immediately after the operation, the shoulder is fitted with an abduction splint for 6 weeks. Postoperative physiotherapy starts from the first day, performing only passive mobilization during these first 6 weeks. The abduction splint is removed after 6 weeks and active mobility is started. After three months, gradual strengthening exercises are started, and after 6 months unrestricted strengthening exercises can be introduced.
Results
According to Gerber(13), pain, mobility and function improved after the open surgical technique. Seventy-four percent of the patients considered the outcome to be good or excellent at 10 years, and most of them reported high degrees of satisfaction and a willingness to undergo the surgery again. In this study, the patients presented a postoperative mean subjective shoulder value (SSV) of 70%, and active external rotation improved 18º to 30º. In addition, active elevation improved significantly at 10 years of follow-up, with an average of over 120º. Thirty-two patients presented an increase in SSV of over 30%, and only 14 patients had an increase in SSV of less than 30%, considering the outcome to be unsatisfactory. Those patients with a poor outcome had more fatty degeneration of the teres minor, and a higher incidence of subscapularis insufficiency and of latissimus dorsi muscle inactivation. Despite the important improvements observed in terms of range of motion and pain, the gain in strength after tendon transfer is low: approximately 40% in women and 25% in men, in relation to the preoperative levels(13).
It has been reported that primary surgeries afford better results than revision surgeries(30). In addition, some authors have reported better outcomes in younger patients(24).
With regard to the surgical approach used, the literature offers no solid statistical data allowing valid comparisons to be made between single and double incision, though it has been reported that the results obtained with a single incision are comparable to those of the standard double incision technique. It has been reported that arthroscopy-assisted techniques afford results comparable to those of open transfer surgery(31).
Another factor that may influence the postoperative results is patient compliance and adherence to a strict physiotherapy regimen, needed to develop neuromuscular control for recruiting the latissimus dorsi as an external rotator instead of an internal rotator(32).
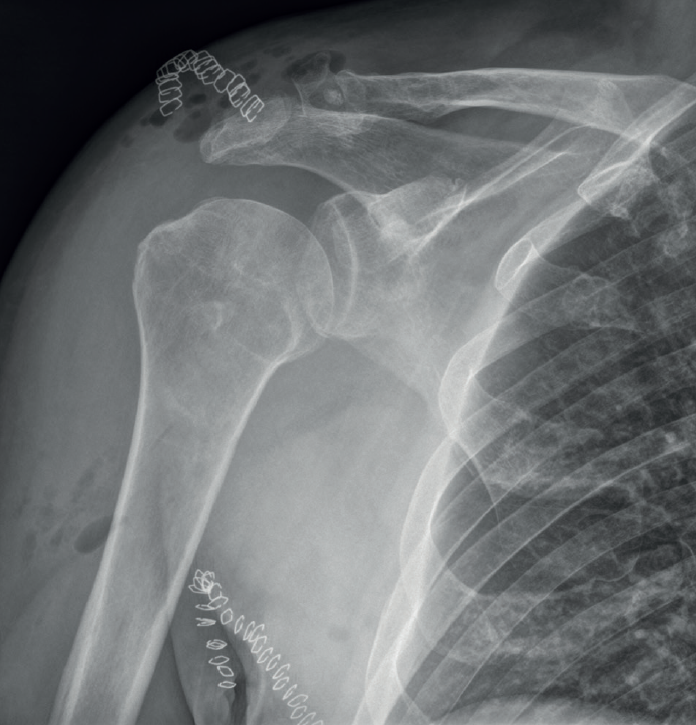
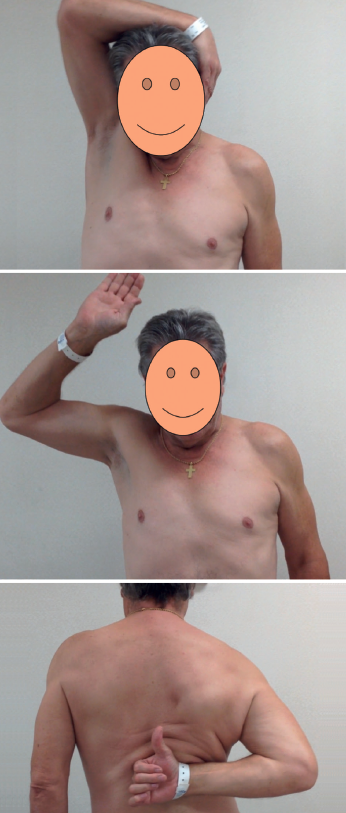
After transfer of the latissimus dorsi, arthrotic degeneration of the joint is comparable to that seen with non-surgical treatment, though progression is slower, and the increase is limited to 1 or 2 stages of the classification of Hamada(13)(Figures 4 and 5).
The incidence of complications of both the arthroscopic and the open techniques is low and includes postoperative hematoma, frozen shoulder, nerve damage, infection, and rupture of the transferred tendon(31).
Transfer of the lower trapezius
Traditionally, transfer of the latissimus dorsi has been regarded as the gold standard transfer in irreparable posterosuperior rotator cuff ruptures, and for several decades it has been used to treat these lesions, with good outcomes in terms of pain and function over the middle and long term.
Transfer of the lower trapezius was initially described for the treatment of brachial paralysis and paralytic shoulder, affording clear improvement in restoring external rotation in these patients(33,34,35). Based on these promising results, this type of transfer began to be used for treating irreparable posterosuperior rotator cuff rupture, employing the Achilles tendon as augmentation measure. At present, transfer of the lower trapezius has become consolidated as a very good treatment alternative in irreparable posterosuperior rotator cuff rupture, improving pain, range of motion and function of the shoulder(36).
The first results of transfer of the lower trapezius for treating massive posterosuperior rotator cuff rupture were published in 2016(37), with a mean follow-up of 47 months. In this study not only did the patients report improvements in terms of pain and range of motion, with an increase in the scores of all the applied scales, but recovery of function was also observed in patients with pseudo-paralytic shoulder.
Different biomechanical studies(38,39,40) have shown that transfer of the lower trapezius affords better leverage in external rotation than transfer of the latissimus dorsi, and is better able to restore the kinematics of the native glenohumeral joint. A recent biomechanical study has compared both transfers and has concluded that transfer of the lower trapezius is significantly better in preventing superior displacement of the humeral head and loss of mobility in abduction, compared with transfer of the latissimus dorsi(41).
However, few clinical studies have compared the two transfer techniques to date(42).
A recent study(43) has reviewed and compared patients subjected to transfer of the latissimus dorsi and transfer of the lower trapezius in irreparable posterosuperior ruptures. The authors see a potential advantage in the fact that the lower trapezius contracts during external rotation and abduction of the shoulder, in contrast to what happens with the latissimus dorsi, which is an internal rotator and abductor of the shoulder. This circumstance would allow better restoration of shoulder kinematics and better outcomes with the lower trapezius, as well as significantly contribute to stabilization of the scapula.
Another advantage of the lower trapezius versus the latissimus dorsi in relation to this transfer is its anatomy. The lower trapezius originates from the thoracic midline to T12, and inserts in the medial 4 cm of the scapular spine(44). Once transferred to the footprint of the supraspinatus, its traction line is very similar to that of the infraspinatus(45). In addition to its anatomical advantage, the trapezius is characterized by simple "learning" of its function once transferred, and this allows for faster recovery(46).
Nevertheless, transfer of the lower trapezius has two possible disadvantages. On one hand, augmentation with autograft or allograft is required, and this increases the costs, the surgery time and morbidity (in the case of autografts) of the process, and implies a risk of failure of graft fixation to the humerus and trapezius. On the other hand, deinsertion of the lower trapezius from the scapular spine could favor a degree of scapulothoracic dyskinesia.
Thus, due to its anatomy, its excursion and traction line much more similar to that of the infraspinatus, the lower trapezius has become the preferred option for many authors in treating massive posterosuperior ruptures, where the loss of external rotation is significant. In summary, according to these authors, the potential advantages of the lower trapezius versus the latissimus dorsi in application to irreparable rotator cuff ruptures are:
- A more cranial origin, with a traction line similar to that of the infraspinatus.
- Excursion and tension similar to that of the infraspinatus.
- The lower trapezius contracts during external rotation of the shoulder, acting as an agonist in external rotation(47).
Indications of transfer of the lower trapezius
The main objective of transfer of the lower trapezius is to restore flexion, external rotation and strength of the shoulder. The ideal patient in this respect is a young individual (under 65 years of age) with shoulder pain, loss of strength and active functional limitation in flexion and/or external rotation, with irreparable posterosuperior rotator cuff ruptures (with fatty infiltration of the supra- and infraspinatus corresponding to Goutallier grades 3-4), in the absence of glenohumeral osteoarthritis (Hamada < 3).
A number of doubts are raised regarding the indications and contraindications in certain clinical scenarios, and which we will address below in question-answer format.
Can transfer of the lower trapezius be made with a damaged subscapularis? Yes, provided the subscapularis can be repaired. Elhassan reported satisfactory outcomes in patients with a positive lift-off test and belly-press test on carrying out repair of the subscapularis and transfer of the lower trapezius(48,49,50).
Can transfer of the lower trapezius be made with a damaged teres minor? Transfer of the lower trapezius can be made with a damaged teres minor, though the outcomes are better if the latter muscle is preserved(48,51).
Can transfer of the lower trapezius be made with pseudo-paralytic shoulder? Elhassan et al.(33) recorded better results in patients starting from an anterior elevation of over 60º, with no glenohumeral osteoarthrosis or only minimal osteoarthrosis, and an evolution of under three years between symptoms onset and treatment. These authors consider that genuine pseudo-paralytic shoulder is a predictor of poor clinical outcomes. In this regard, genuine pseudo-paralytic shoulder is considered to be a shoulder with an anterior flexion deficit of less than 60º and abduction less than 60º during at least 6 months, with no improvement of range of motion after eliminating the pain through the infiltration of local anesthetic.
Thus, the absolute contraindications of transfer of the lower trapezius are:
- Paralysis of the lower trapezius.
- Active infection of the soft tissues or shoulder.
- The relative contraindications of transfer of the lower trapezius are:
- Pseudo-paralysis with elevation < 60º.
- Complete subscapularis rupture with superior escape of the humeral head.
One of the most important aspects to be taken into account when proposing transfer of the lower trapezius is that the patient must be convinced and motivated, as well as cooperative, since the postoperative period is long, with prolonged immobilization in external rotation for 6 weeks, and with a prolonged rehabilitation program. Patient failure to comply with such immobilization for 6 weeks will result in loss of tension of the plasty, and the functional outcomes probably will not be as desired.
It is also very important for the patient to strengthen the lower trapezius, as well as the rest of the periscapular muscles, before surgery is carried out. This will allow for optimum results. The patients are instructed to do external rotation against resistance exercises with the arm in adduction. A series of daily exercises during four weeks before surgery is enough.
One of the inconveniences of using the lower trapezius is that it needs a graft to reach the insertion. As a result, complications related to the graft could add to those inherent to the surgery itself. The allograft most often used in these transfers is the Achilles tendon. Some authors propose the use of a semitendinosus autograft instead of an Achilles allograft, in order to avoid the possible complications related to use of an allograft.
Surgical technique
The initial surgical technique described by Elhassan placed the patient in lateral decubitus, performing an osteotomy of the acromion to access the rotator cuff. The technique was subsequently modified, changing the patient to the deck chair position and adopting arthroscopic techniques for tendon reinsertion in the humerus - thus preserving the fibers of the deltoid muscle and avoiding osteotomy of the acromion. Arthroscopic tendon reinsertion has demonstrated better results than the classical open techniques; we therefore recommend its use in this type of transfer(42).
The surgical technique is described further on in another chapter of this monograph, so we will not address it in detail here.
During the postoperative period, the patient must keep the shoulder immobilized in external rotation with an orthosis for 6-8 weeks, and can only remove it for personal hygiene, maintaining the passive external rotation. From week six, assisted passive and active exercises are started, with a gradual increase in their intensity.
The possible complications of transfer of the lower trapezius are fundamentally two. The first, as already described by Elhassan(37), is the fact that some patients develop scapular dyskinesia following deinsertion of the lower trapezius from the scapular spine. The second complication is related to the fact that this is an indirect transfer, and thus the graft may fail at its insertion in the greater tuberosity, at middle level, or at its junction with the lower trapezius.
The technique is reproducible, with few complications, and is easier to perform than the latissimus dorsi procedure in obese patients. Furthermore, as also occurs with transfer of the latissimus dorsi, it may allow future reverse replacement if needed(27,52).
However, transfer of the lower trapezius is a relatively new technique, and long term studies are therefore needed to confirm the validity of the procedure. Comparative trials involving larger patient samples and longer follow-up periods are required to better understand the indications of this type of transfer as treatment for this disease condition.
Conclusions
Tendon transfers for the treatment of irreparable posterosuperior rotator cuff ruptures in patients with disabling loss of active external rotation, whether associated or not to loss of elevation of the shoulder, and without glenohumeral osteoarthritis, are demanding and complex procedures that can restore shoulder function and alleviate pain. In addition, they can help restore part of the strength, though this improvement should not be expected to be significant.
Candidate patients must be able to comply with long rehabilitation protocols and should be informed about the benefits to be expected after the operation. In this respect, the patient expectations must coincide with the predicted outcomes.
The long term failure rate is low and does not close the door to rescue surgery in the form or reverse replacement.
Careful patient selection is very important for the success of this surgery.




