Introduction
Reconstruction of the anterior cruciate ligament (ACL) is one of the most frequent arthroscopic surgeries in sports traumatology. Nevertheless, there is still considerable debate regarding the ideal type of graft and the initial fixation technique of the graft.
In our setting, most reconstructions are now made using two tendons of the pes anserinus (goose foot) - semitendinosus and gracilis - which conform a four-fascicle plasty when doubled onto themselves. The tendon of the semitendinosus can also be doubled onto itself three or four times to obtain a graft of similar resistance, sacrificing a single tendon structure in exchange for a much shorter plasty(1).
Ideally, fixation should afford resistance to translation of the graft and maintain its qualities during the initial postoperative phase. An interference screw is commonly used in the tibia(2). However, its positioning in the tibial tunnel could place it in a biomechanically inferior position(3), and its use in short grafts may be particularly problematic(4,5).
Fixation alternatives have been investigated, supplementing intra-tunnel positioning of the interference screw with another extracortical system (metal staples or plates onto which the sutures are knotted) or directly resorting to screwless extracortical suspension systems. Nevertheless, fixation performed only with extracortical systems can also pose inconveniences, such as lesser translation resistance(6) or an increased risk of osteolysis and the formation of cystic collections secondary to joint fluid leakage(7). The supplementing of intra-tunnel fixation with extracortical support systems based on guide suture traction, such as PushLock® (Arthrex®), may significantly increase the maximum resistance of the fixation(8). In addition, the use of high-resistance suture systems for the tendon extremities, such as FiberLink® or GraftLink® (Arthrex®), may modify the final characteristics of the assembly.
Such supplementing is of capital importance for the outcome of surgery, in view of the risk that tibial fixation with interferential screws may not be enough to resist exposure to the repeated cyclic loads of daily activities and early rehabilitation(9,10). The hypothesis raised is that the fixation obtained by knotting the braided sutures of the graft onto a simple bone bridge on the anterior cortical component of the tibia could satisfactorily supplement fixation with conventional interferential screws, without having to use other extracortical elements. The aim is to determine whether the dual stabilization models improve upon the reliability of the simple models, and whether there are significant differences between the two tested duplication systems.
Material and methods
A mechanical study was made of the traction resistance of four fixation models involving bioequivalent tendon grafts (bovine digital extensors) introduced in porcine tibial bone:
- Model A: simple guide suture knotting at tunnel exit over a cortical bridge.
- Model B: interference screw of the same diameter as the tunnel.
- Model C: combination of interference screw with supplementing of guide suture fixation by knotting over a simple bone bridge.
- Model D: combination of the mentioned screw with a second fixation of the guide sutures to a PushLock® (Arthrex®) anchoring.
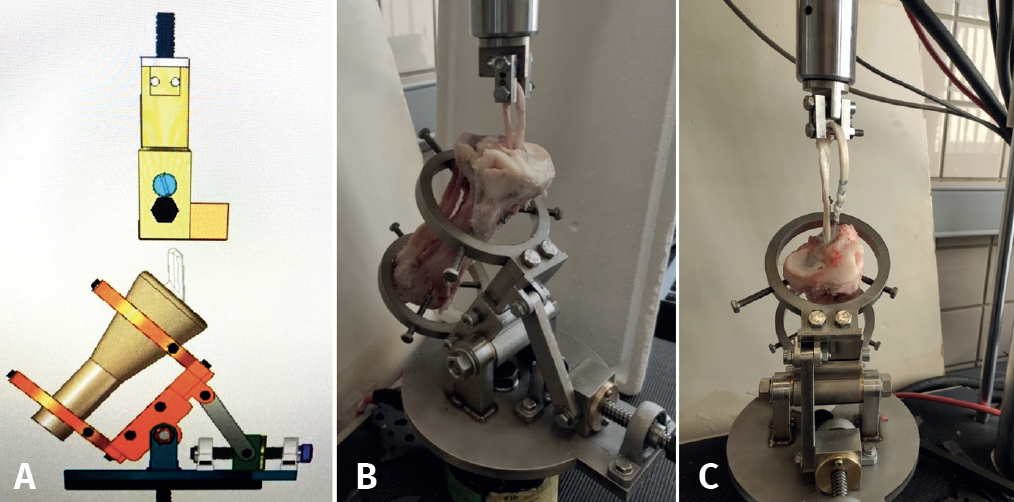
Use was made of a traction-compression test machine (MTS Mini Bionix 858®) with a loading capacity of up to 15 kN and equipped with a loading cell of 5 kN, with connecting elements specifically deigned for our study. The elements used are shown in Figure 1, and allow connection of the anatomical models to the traction-compression test machine, with the application of traction loads of up to 2 kN.
The bone and tendon specimens were kept frozen at − 20 °C, which has been shown in previous studies to not significantly affect their mechanical characteristics(11). Based on the literature review and in order to obtain a sufficiently representative sample, we included 6 specimens for each study group.
Following their extraction and quadruple braiding with loop-type high-resistance suture (FiberLoop #2®), the bovine extensors conformed bifascicular plasties measuring 8.5 mm in mean diameter in both groups, followed by porcine tibial tunnel preparation using a surgical technique similar to that employed in humans. For this purpose we used a variable-angle tibial perforation guide (Arthrex®), establishing a standard angle of 55° and employing a 9-mm anterograde drill.
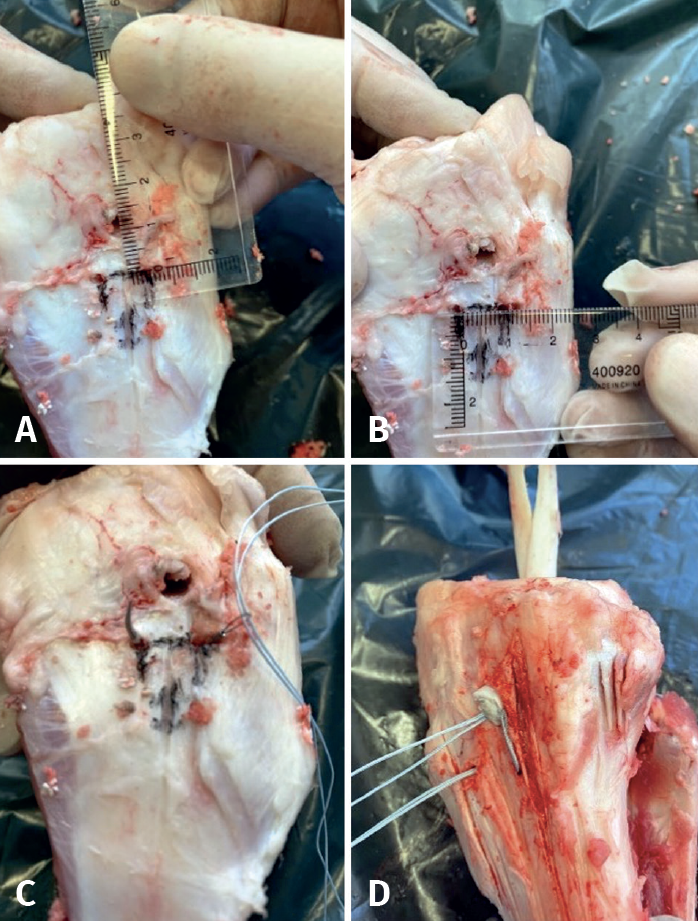
In group A, plasty fixation was made by systematically knotting the extremities of the high-resistance tendon suture. As shown in Figure 2, the tibial cortical bone is perforated twice at 1 cm from the extraarticular exit of the tunnel, with each perforation in turn separated 1 cm and in a confluent direction to allow the passing of a atraumatic needle. Two suture extremities from one tendon end were passed and knotted to the other two extremities of the other end via four simple knots (two of them inverted).
In the second group fixation of the construct was carried out by simple screwing with a BioComposite® 9 × 23 mm (Arthrex®) interference screw, ensuring cortical contact at its distal extremity.
The third sextet of specimens combined both fixations, with equivalent screwing plus an extra knot of the guide sutures over the bone bridge.
Lastly, in the fourth group dual fixation was likewise carried out, with screwing and subsequent tightening of the guide sutures to a PushLock® (Arthrex®) anchoring distal to the tunnel. This implant allowed threading of the sutures in its interior and adjustment of their tension during final positioning of the anchoring.
Once prepared as described above, the specimens were placed in the test machine with a hook-type device positioned in line with the tibial tunnel. The contemplated model of mechanical analysis reproduced that already used by other authors(12), with the aim of being able to compare the results obtained.
A small 5 N preload was manually applied to each sample, followed by a constant load of 40 N during 70 seconds. Then, the mechanical cyclic loading test was carried out, comprising 500 cycles at between 100 and 200 N at a frequency of 1 Hz. The models that survived this cyclic test were subjected to traction until specimen failure at 20 mm per minute. The data loading and displacement data were recorded at 512 Hz.
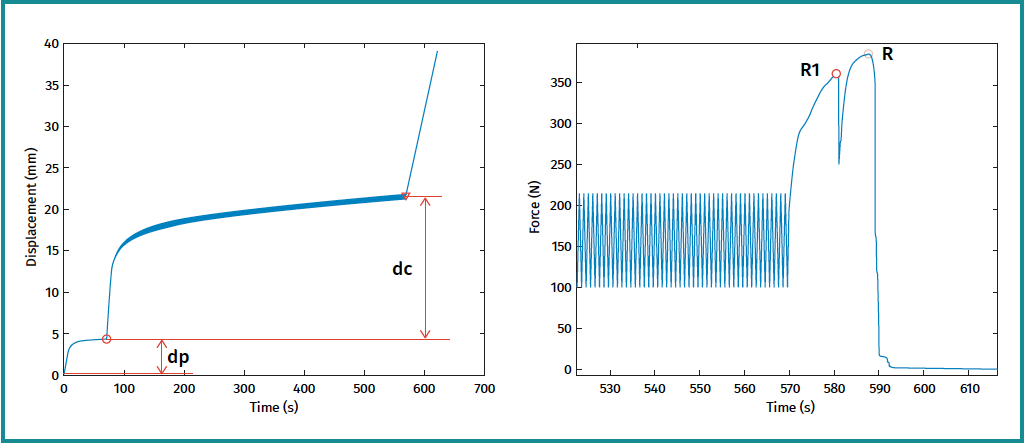
The following were calculated for the graft-bone-fixation system as outcomes of the test (Figure 3):
- Displacement during preload (or dp), which is the difference (in mm) between the intraarticular length at the start and end of preconditioning.
- Displacement during cycling (or dc), which is the difference (in mm) between the intraarticular length after preconditioning and that recorded after the cyclic test, in both cases with the fixation subjected to the minimum traction load (40 N).
- Last load in the rupture test or maximum rupture load, R(N).
- Maximum rupture load (first local maximum), R1(N), defined as the force at the first point of the load-displacement curve where the slope clearly decreases.
- The failure mode of each specimen was recorded.
The results obtained were analyzed using the SPSS® version 28 statistical package (IBM®, Chicago, IL, USA). The mean ± standard deviation (SD) of the variables was calculated for each group. Differences between groups were evaluated by one-way analysis of variance (ANOVA) for independent data, with significance being established for p < 0.05. The Fisher exact test in turn was used for the comparison of dichotomic variables.
Results
In group A, corresponding to fixation using high-resistance suture with a bone bridge, all the specimens passed the cyclic loading rest and reached the last tension phase to the point of rupture.
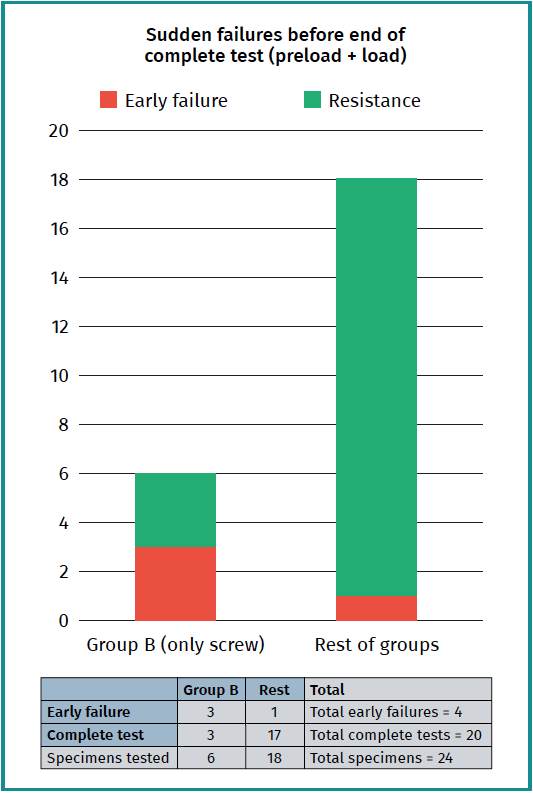
In group B, corresponding to the simple interference screw fixation group, three of the 6 specimens failed during the cyclic tension process after 45, 116 and 467 cycles, respectively.
In group C, corresponding to the dual screw-knotting to bone bridge fixation group, a single early acute failure was recorded after 181 cycles, while in group D all the specimens correctly resisted the full evaluation. All the specimens that failed in one moment or other did so due to rupture of the suture (Figure 1C) or translation of the tibial fixation, with no case of rupture of the graft tissue itself or of the bone bridge.
A statistically significant relationship was observed between single fixation with an interference screw and the occurrence of sudden failures during the cyclic phase of the test (p = 0.035) (Figure 4).
After the preloading or conditioning phase, the mean magnitude of displacement of the graft (dp) was 3.60 ± 1.17 mm in the transosseous suture fixation group, 1.82 ± 0.49 mm in the bio-interference screw group, 1.93 ± 0.38 in the interference + transosseous suture group, and 2.04 ± 0.42 in the interference + PushLock® group. In relation to the above, the one-way ANOVA revealed a statistically significant difference between at least two of the groups (F = 8.718; p < 0.001), and the subsequent multiple analysis with the Tukey HSD test evidenced significant differences between groups A-B, A-C and A-D (p < 0.01), but not between groups B-C, B-D or C-D (Figure 5).
In the cyclic loading phase, the mean magnitude of displacement of the graft (dc) was 15.20 ± 3.47 mm in sextet A, 3.50 ± 1.05 mm in the group of survivors for the interference screw (those that completed the entire cyclic loading phase), 4.45 ± 0.83 in the 5 survivors of the interference + transosseous suture group, and 4.94 ± 1.06 in the interference + PushLock® group. The same statistical significance indicated above was seen to be repeated in both the statistical analysis of translation during cycling and the analysis of global preload-load translation. The one-way ANOVA (F = 36.813; p < 0.001; and F= 49.696, p < 0.001) and the Tukey post hoc analysis revealed statistically significant differences between groups A-B, A-C and A-D (p < 0.01), but not between groups B-C, B-D or C-D (Figure 5).
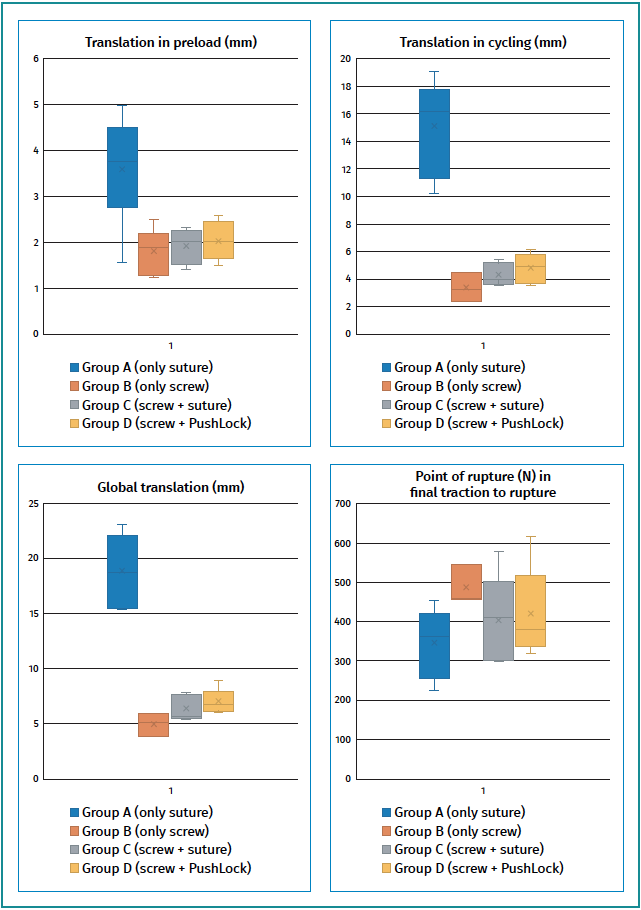
In the last phase, corresponding to maximum resistance (to rupture) testing, the first group comprising suture to bone bridge failed at a mean value of 369.75 ± 92.93 N. In the second group, corresponding survivors with the interference screw, the mean resistance reached 519.6 ± 54.42 N. In the third group (interference + transosseous) the value reached was 430.34 ± 122.61 N, and in the fourth group (interference + anchoring) the value was 448.86 ± 120.33 N. There were no statistically significant differences between the different fixations at the level of significance considered (one-way ANOVA; F = 1.409; p = 0.276) (Figure 5).
Discussion
Considering a load of 450 N as the upper limit which the ACL can be expected to support in the course of daily activities(8), and a load of 200 N as an intermediate value associated to the maximum load which the graft will support in a postoperative period with accelerated rehabilitation protocols(13), our study evidences that deficient fixation is possible, with a risk of excessive tibial translation of the graft in up to 50% of the cases. The results of the present experimental study reinforce the current notion(8,14) that the fixation of tendinous plasties for reconstruction of the ACL with simple bio-interference screws may not be enough to resist the estimated forces inherent to early rehabilitation.
On the other hand, our alternative option without specific fixation material, with single fixation involving a tibial cortical tunnel and the knotting of high-resistance sutures, could offer theoretical advantages in the form of cost reductions (this being particularly interesting in centers with fewer resources) and the absence of interference of the osteosynthesis material in young patients with open physes. However, our study points to greater insufficiency of the tibial fixation, with intolerable mean translations of 1.5 cm. The behavior of this group was more uniform, in all cases reaching the final phase of the biomechanical study, but the maximum resistance only reached the standards we regard as acceptable in one-third of the cases.
Thus, we consider that the mentioned theoretical advantages of this system of knotting over cortical bone are probably incompatible, when used as a single technique, with the postoperative protocols currently applied in clinical practice.
Dual tibial fixation corresponding to groups C and D did not increase maximum traction resistance versus the specimens in group B (only bio-interference screw), which survived the entire process, but did reduce the failure rate, with the recording of only one acute failure in the 12 specimens (8.33%) - none involving the combination screw-PushLock®. However, we found no statistically significant differences between the two dual alternatives considered. A further study involving a larger sample size in order to increase the statistical power is probably needed. Since the preparation of specimens and their study using the device constructed for this purpose for the MTS Mini Bionix proved easily reproducible, the possibility exists of continuing the study independently of the tibial fixation of the plasties of the ACL with the contemplated dual systems, as well as other devices currently found on the market.
Tibial fixations of grafts for the ACL with knotting over a bone bridge and using simple interference screws are not equivalent, though in both circumstances they seem insufficient due to different reasons. Moreover, in none of the cases did loading limitation occur because the maximum resistance of the substituting graft fibers had been reached; rather, the fixation failed before the tendon structure was damaged, as a consequence of suture rupture or due to massive translation of the plasty. We thus believe it to be feasible to largely increase the safety of the reconstruction by supplementing or performing tibial fixation in dual fashion by adding an extra anchoring or by using our proposed transosseous suture.
The experiment carried out involved the use of animal models that are considered to be bioequivalent to ACL plasty in humans, with the added advantage of using tissues with uniform characteristics in terms of breed, weight and age. However, it must be taken into account that the study only reports on the behavior of the models under a certain mechanical stress, which might not precisely reflect the reality of the patient postoperative period. It also must be taken into account that satisfactory reconstruction of the ruptured ACL is dependent not only on local mechanical factors but also on more extensive biomechanical aspects and particularly biological factors, which are not the subject of this study.
Conclusions
In the present experimental study, single tibial fixation of the tendon plasty with a bio-interference screw proved unsatisfactory, with a statistically significant incidence of excessive graft translation.
From the statistical perspective, dual tibial fixation did not significantly modify maximum traction resistance, though it did reduce the incidence of sudden failure due to translation.
No differences were found between the two dual fixation alternatives studied. Thus, due to its simplicity, we recommend the interference screw combined with guide suture knotting in a simple bone bridge.
Level of evidence
Level I, randomized control study in specimens of animal origin.
Clinical relevance
This study increases the scientific evidence on the possible insufficiency of single tibial fixation in reconstruction of the ACL - the option currently most often chosen by orthopedic surgeons. These data could lie behind some failures of tibial fixation or impingement of plasties as a result of their intraarticular elongation. The current study moreover paves the way for new biomechanical studies for improving the reliability of our surgeries.




